|
October 8, 2022
While Studies Showed The Vaxxes And Boosters Were Killing People, Another Study Showed Vitamin D Was Helping People Stay Alive! Staying Well Informed Is The Key To Staying Healthy
By Dr. Joel S Hirschhorn for All News Pipeline
Best article on vitamin D
I cannot emphasize enough that using enough vitamin D supplementation is absolutely critical for fighting COVID and many other infections and medical problems. Not only should you read the following article, which is long and complex, but you also need to convince others about the importance of vitamin D. This article provides many details on how to use vitamin D and how it protects your health.
Rapidly Increasing Serum 25(OH)D Boosts the Immune System, against Infections—Sepsis and COVID-19
Conclusions
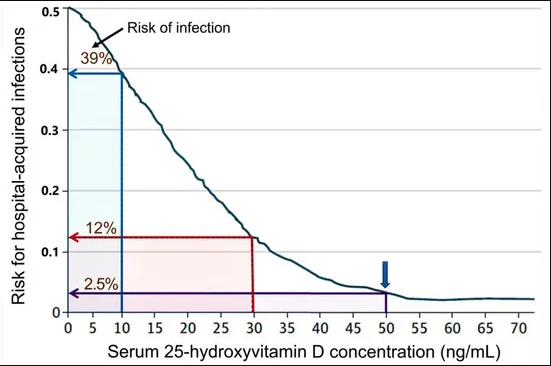
A robust immune system is essential to overcome infections without complications. It depends on the adequate entry of vitamin D3 and 25(OH)D into immune cells for generating calcitriol. The latter required maintaining a serum 25(OH)D concentration of over 50 ng/mL. Therefore, to successfully manage and overcome an infectious epidemic or a pandemic, it is crucial to maintain the population’s serum 25(OH)D concentration above the mentioned therapeutic level.
In acutely ill persons, especially those with vitamin D deficiency having infections, raising serum D3 and 25(OH)D concentrations quickly is paramount and life-saving. In these urgent situations, 0.5 to 1.0 mg of calcifediol can raise serum 25(OH)D concentrations above the minimum therapeutic levels of 50 ng/mL in four hours and boosts the immune system within a day that facilitates to overcome infections.
While calcifediol raises serum 25(OH)D within hours, the oral administration of even high doses of vitamin D takes three to five days to raise serum 25(OH)D concentrations. This delay is due to its less efficient absorption than calcifediol and the need for vitamin D to undergo 25-hydroxylation in the liver, a rate-limiting step. In acutely ill patients, as in those in the ICU, administering even high doses of oral D3 may take a week to increase serum 25(OH)D concentration. Therefore, it is unhelpful in emergencies like SARS-CoV-2 infections.
With a weight-based, single dose of calcifediol, as described in Table 3, circulatory 25(OH)D concentrations are maintained for approximately 8 to 14 days. In contrast, parental high dose vitamin D3, administered as loading or bolus, will maintain serum 25(OH)D concentrations between two to three months. Although the circulatory half-life of D3 is short, due to the larger initial doses, it maintains a higher circulatory concentration of both D3 and 25(OH)D for several weeks—partly because of the release from the storage in fat and muscle tissues.
Therefore, with calcifediol, one should administer a suitable higher dose of vitamin D3. This can be done using 50,000 IU vitamin D capsules in outpatients’ setups and emergencies, as illustrated in Table 3. Nevertheless, considering the non-genomic beneficial actions of vitamin D3 and its longer duration of physiological actions described above, the combination of D3 and calcifediol provides better clinical outcomes than either alone. Therefore, administering the proper doses of D3 and calcifediol is recommended for patients with infections as an adjunct therapy at the first outpatient or inpatient encounter.
  Multiple observational and RCTs have demonstrated that serum 25(OH)D concentrations (pre-infection or on admission) inversely correlated with the incidence, severity, and rates of death from COVID-19. Meanwhile, vitamin D supplementation significantly reduces complications and deaths. Irrespective of the regimen, initial bolus or loading doses of vitamin D and/or calcifediol should follow a daily or weekly, longer-term maintenance regimen.
The described schedules in the three tables are highly cost-effective ways to raise serum 25(OH)D concentrations and maintain it to keep the immune system on high alert. Consequently, it prevents and/or reduces infections and complications from COVID-19 and other infections. For non-obese 70 kg adults, the recommended longer-term vitamin D3 maintenance dose is 5000 IU/(0.125 µg) day or 50,000 IU (1.25 mg)/week (or every ten days). Nevertheless, this regimen takes a few months to reach the desired serum 25(OH)D concentration above 50 ng/mL. It can be expedited by ingesting vitamin D, 10,000 IU/day (250 µg/day) for 8 to 10 weeks and reverting to the daily dose of 5000 IU.
Rectifying vitamin D deficiency costs less than 0.1% of the costs related to evaluating and treating comorbidities and complications associated with vitamin D deficiency. For example, in western countries, vitamin D supplementation to maintain serum 25(OH)D costs approximately $8 per person/year, versus an average cost of $5000 to $15,000/year per person to manage vitamin D deficiency-associated diseases and related complications.
Despite a favorable cost-benefit ratio, availability as a non-prescription over-the-counter nutrient, and exemplary safety profile, millions of people become ill due to vitamin D deficiency requiring medical attention, markedly increasing the cost of healthcare. Vitamin D deficiency increases healthcare costs, absenteeism and opportunity costs and reduces productivity.
Considering the described significant benefits associated with disease prevention, reduced illness severity, reduced absenteeism, complications and deaths, improved well-being and higher productivity, the calculated overall cost-benefit ratio for administered vitamin D3 supplements exceeds 1 in 20,000.
Despite these data, no country is yet to recommend vitamin D (or has published proper guidelines with the right doses) for disease prevention or recommended it as an adjunct therapy to prevent complications and deaths from infections or other diseases. This report provides rationale, justifications, straightforward guidance, and practical tables that provide regimens for use in clinical practice for achieving and maintaining the serum 25(OH)D concentrations needed to ensure a robust immune system that helps to overcome infections, including SARS-CoV-2.
(ANP FUNDRAISER: Due to heavy censorship by 'big tech' upon ANP articles, we're running a fundraising drive. We also want to thank everybody who has donated to ANP over the years. With donations and ad revenue all that keep ANP online, if you're able, please consider donating to ANP to help keep us in this fight for America's future at this absolutely critical time in US history. During a time of systematic, 'big tech' censorship and widespread institutional corruption, truth-seeking media and alternative views are crucial, and EVERY little bit helps more than you could know!)
Excellent article on COVID boosters
Rapid Rollout of New COVID Boosters With No Human Trials — ‘A Tale of Recklessness’
Summary:
- The U.S. Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention (CDC) cooperated to issue Emergency Use Authorizations (EUA) and roll out new, bivalent Pfizer and Moderna COVID-19 vaccines this week, without any human trials, which is unprecedented.
- There is international coordination regarding bivalent boosters, and a major effort will be undertaken to get them into arms, despite historically low levels of severe COVID-19. Why?
- These vaccines continue to enjoy extraordinary protection from liability, while the recipient has no access to the legal system in the case of injury.
- There is no evidence the new vaccines are safe, while there is limited evidence that they may be more harmful than earlier COVID-19 vaccines. However, in the absence of human testing, there is no way to truly predict their safety. Safety data are being concealed by federal health agencies. Messaging by them is misleading.
- There is no evidence the new bivalent vaccines will be more effective than the older vaccines, and existing evidence suggests that any efficacy they provide will persist no longer than one to several months.
- COVID-19 vaccines appear to increase susceptibility to COVID-19 infections, on average starting six months after inoculation.
- Perpetual boosters briefly stave off the negative efficacy that develops a few months after a COVID-19 vaccination. This may be why frequent boosters are being pushed. But frequent boosters may also weaken overall immunity and may even contribute to rising mortality rates in the U.S. and U.K.
ANP FUNDRAISER: With non-stop censorship and 'big tech' attacks upon independent media, donations from readers are absolutely critical in keeping All News Pipeline online. So if you like stories like this, please consider donating to ANP.
All donations are greatly appreciated and will absolutely be used to keep us in this fight for the future of America.
Thank you and God Bless. Susan and Stefan.
PLEASE HELP KEEP ANP ALIVE BY DONATING USING ONE OF THE FOLLOWING METHODS.
One time donations or monthly, via Paypal or Credit Card:

Or https://www.paypal.me/AllNewsPipeLine
OR Donate to ANP via Subscribestar
Donate Via Snail Mail
Checks or money orders made payable to Stefan Stanford or Susan Duclos can be sent to:
P.O. Box 575McHenry, MD. 21541

|